
Urbanisation & Health Outcomes: A Data Led Approach for Accountability and Action
June 2022
by
Lead Author: Josh Artus
Before reading this report please note that we are a non-profit grant and citizen supported lab, we use our funding to create free scientific reports, which provide foundational knowledge about health, health inequities, and health justice. We prioritise the hiring of scientists and researchers from marginalised communities to ensure that the lived experience is covered in an ethical, inclusive, and accurate manner.
Our goal is to be an open lab that is “for the people by the people” and your support helps make that happen.
“Justice is the truth in action.”
- Joseph Joubert, 1754-1824
DESCRIPTION
The truth is that Urbanisation and industrialisation is killing the human race.
Our environments are making us sick and our forefathers got it wrong. Those in the offices of today fail to represent our most basic needs: food and water, sufficient rest, clothing and shelter, overall health, and reproduction.
Our water is contaminated
Our food crops are dwindling, full of toxic chemicals, in broken supply chains and rising in cost.
The costs for shelter rise beyond wages forcing many into homelessness and insecurity.
Zero-contract hours, 24-hr economies, and dense living make rest and sleep difficult.
Our health and wellbeing are deteriorating despite advances in pharmaceutical and diagnostic medicine.
Sperm counts are lowering and the female endocrine system is being attacked.
The action: to use the tools of the time to advance towards justice. To be responsible and accountable for one's own actions. The link between urbanisation and human biology is developing. There is a chance to no longer account for the place a person lives to be a determinant in their health.
How did we get here?
Since the 5th century BC the European man has seen a distinction between land and human.
The human was to dominate the land in order to master his own destiny. This hierarchy turned Land from our kin and healer into a resource. We collectively began to lose the literal life sustaining nutrition from living in harmony with the original environment.
This belief of the dominant man defined colonialism, gave birth to racism, and ultimately led to their successor, capitalism. Ecosystems from Snowdonia to Samoa have been destroyed in the name of man’s supremacy.
This continued into the 20th century as cities became the social, cultural, political and economic heartlands. Sustainability and symbiosis were not the aim and we’re seeing it now in the human health outcomes of urbanisation: the rise of non-communicable diseases; anxiety, depression, PTSD, diabetes, obesity, asthma, cardiovascular disorders, and cancers.
Our systems of governance spend time tracking health outcomes and aim to intervene through urbanisation's ability to ‘create change’ and ‘do good’. However, rarely has it acknowledged, accepted and acted on its own pathways to these diseases. That can change now.

Where we now go
The Biological InEquity Index tracks the environmental data and deprivation trends that are the result of urbanisation:
air pollution (pm2.5),
noise pollution (road, rail, air),
light pollution (radiance at night),
heat (heatwave data),
deprivation statistics.
This index uses neuroscience research into how our stress response system engages with these metrics’ values to paint a picture of whether a given place is high in stressors that increase biological risk. Chronic exposure to these stressors can act as a pathway to dysregulation of our biological systems such as our immune, endocrine and metabolic functions, making us more susceptible to a host of illnesses, disorders and diseases.
Rather than using downstream outcome based data and companies “doing good” policy writers should be responsible for their actions, the accumulation of pollutants, stressors and resources. As a baseline we can add socio-demographic data on top to observe how certain marginalised groups may be at a greater biological inequity that others. This means we can start asking questions such as:
If an area has a propensity to be high in heat stress, what measures are taken to create shade and lower exposure to older people?
If an area is high in air pollution, what efforts are being taken to regulate polluters such as incinerators, factories, and multiple delivery based businesses?
If an area is high in noise pollution, (a) are walls and windows sufficiently insulated to prevent noise from trespassing into homes, impacting pregnant people’s sleep, and (b) what traffic, delivery, urban management and design decisions are being made to lower the noise output levels?
If an area is high in deprivation, what investments can be made through urban development to make marketable differences?
Direct questions about the built environment, that can be changed through urbanisation, and link them to improving health outcomes.
This index gives these people a chance to deliver social impact through the environment and for the rest of us to hold them accountable to the meaningful changes that will no longer make the places we live a predictor of our health outcomes.
It’s time that those within the system start working for the people they claim to be: current and future generations. The solutions to health places are all there, it’s the organising of actions through a framework is what’s needed.
Peter Drucker famously said, “If you can't measure it, you can't manage it.” Well, we can now measure the built environment’s outputs as pathways to population health, so we can now manage it too.
By acting on the truths of human biology and urbanisation we can create justice for all, and for those yet to be born.
Here are some truths from the data at MSOA level for the regions of England, Scotland, and Wales.
-
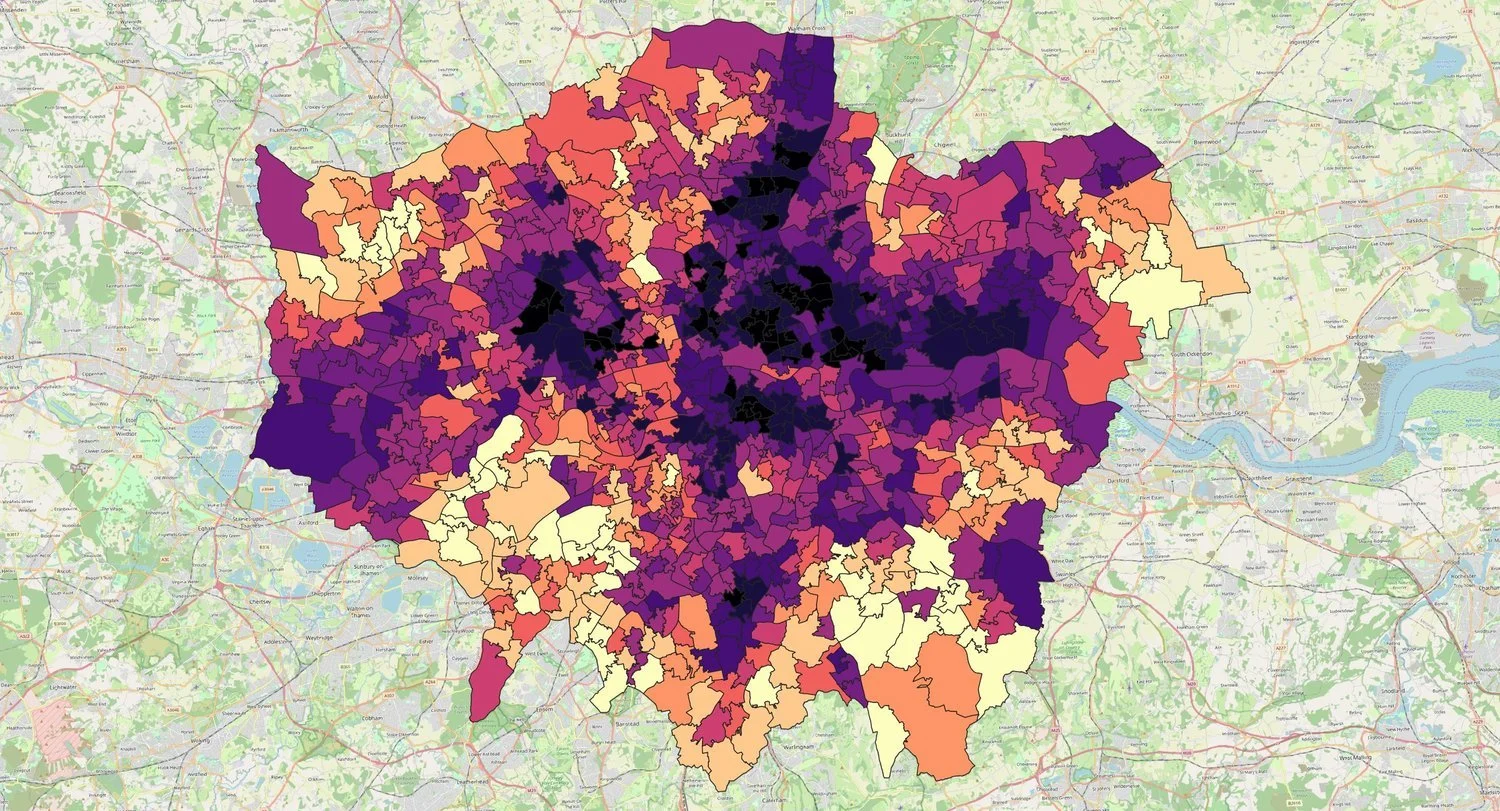
![]()
Top 5 areas of highest biological inequity in London:
St Raphaels, Brent
Hackney Wick, Hackney
Homerton South, Hackney
White Hart Lane, Haringey
Somers Town, Camden
-
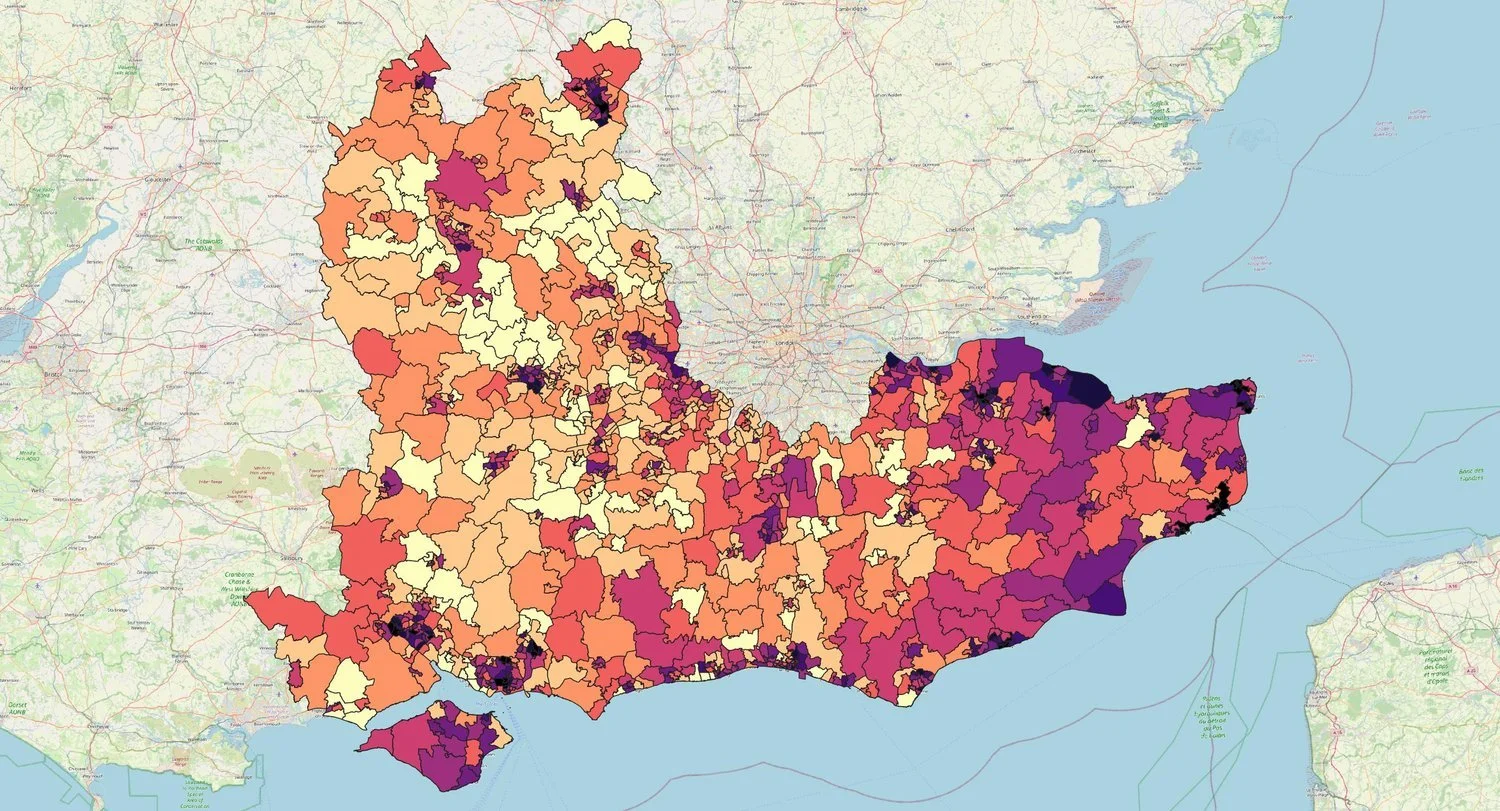
![]()
Top 5 areas of highest biological inequity in the South East:
Margate Town, Thanet
Dane Valley & Northdown Hill, Thanet
Newington, Thanet
Folkestone Harbour, Folkestone and Hythe
Gillingham Central, Medway
-
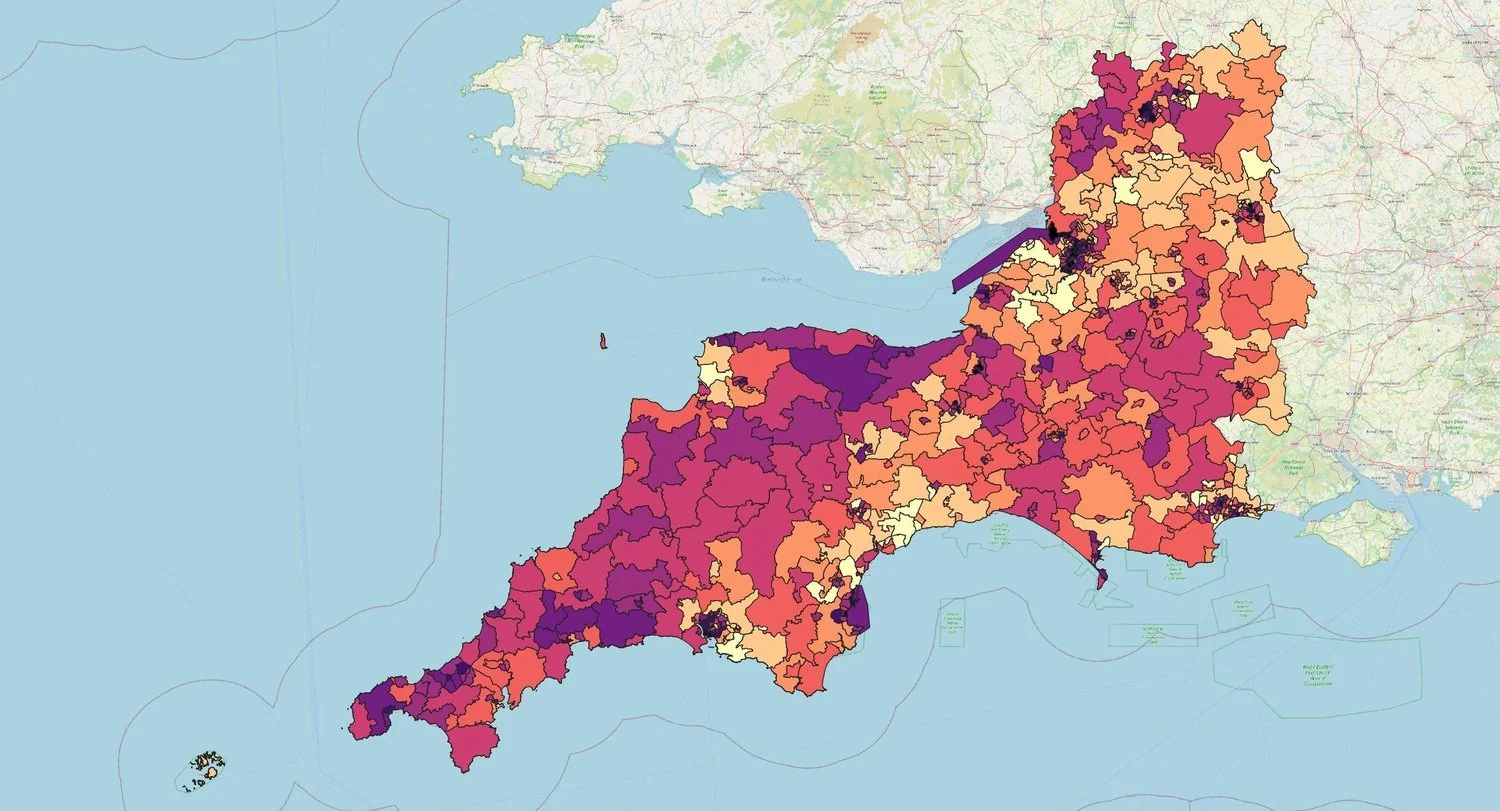
![]()
Top 5 areas of highest biological inequity in the South West:
Temple Meads, Bristol
Barton Hill, Bristol
Lawrence Weston, Bristol
Knowle, Bristol
Knowle West, Bristol
-
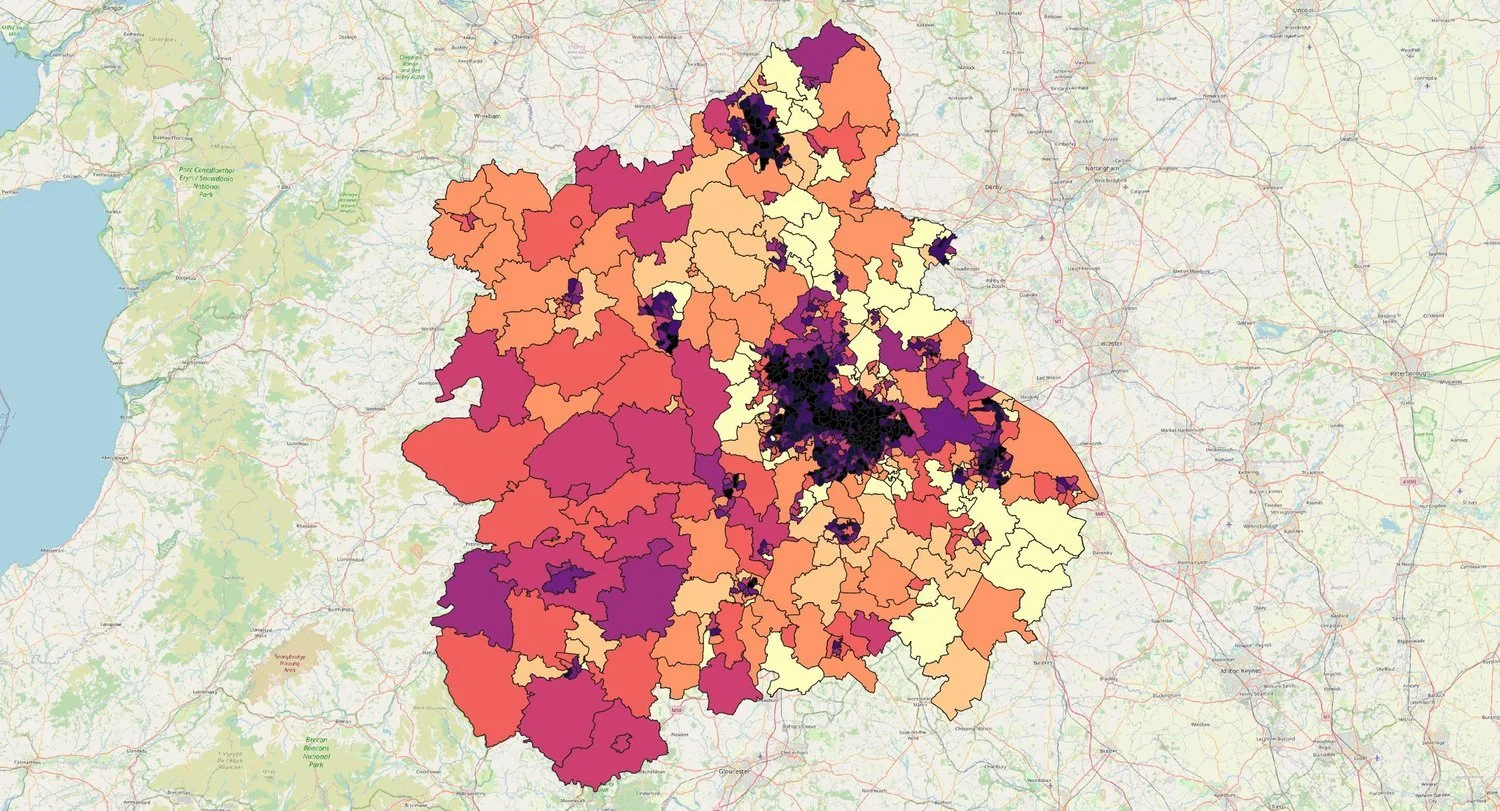
![]()
Top 5 areas of highest biological inequity in the West Midlands:
Castle Vale, Birmingham
Brookvale, Birmingham
Gravelly Hill & South Erdington, Birmingham
Birchfield East, Birmingham
Aston Park, Birmingham
-
![]()
Top 5 areas of highest biological inequity in the East Midlands:
Chaddesden West, Derby
New Normanton, Derby
Rose Hill & Castleward, Derby
Allenton & Osmaston, Derby
St Matthews & Highfields North, Leicester
-
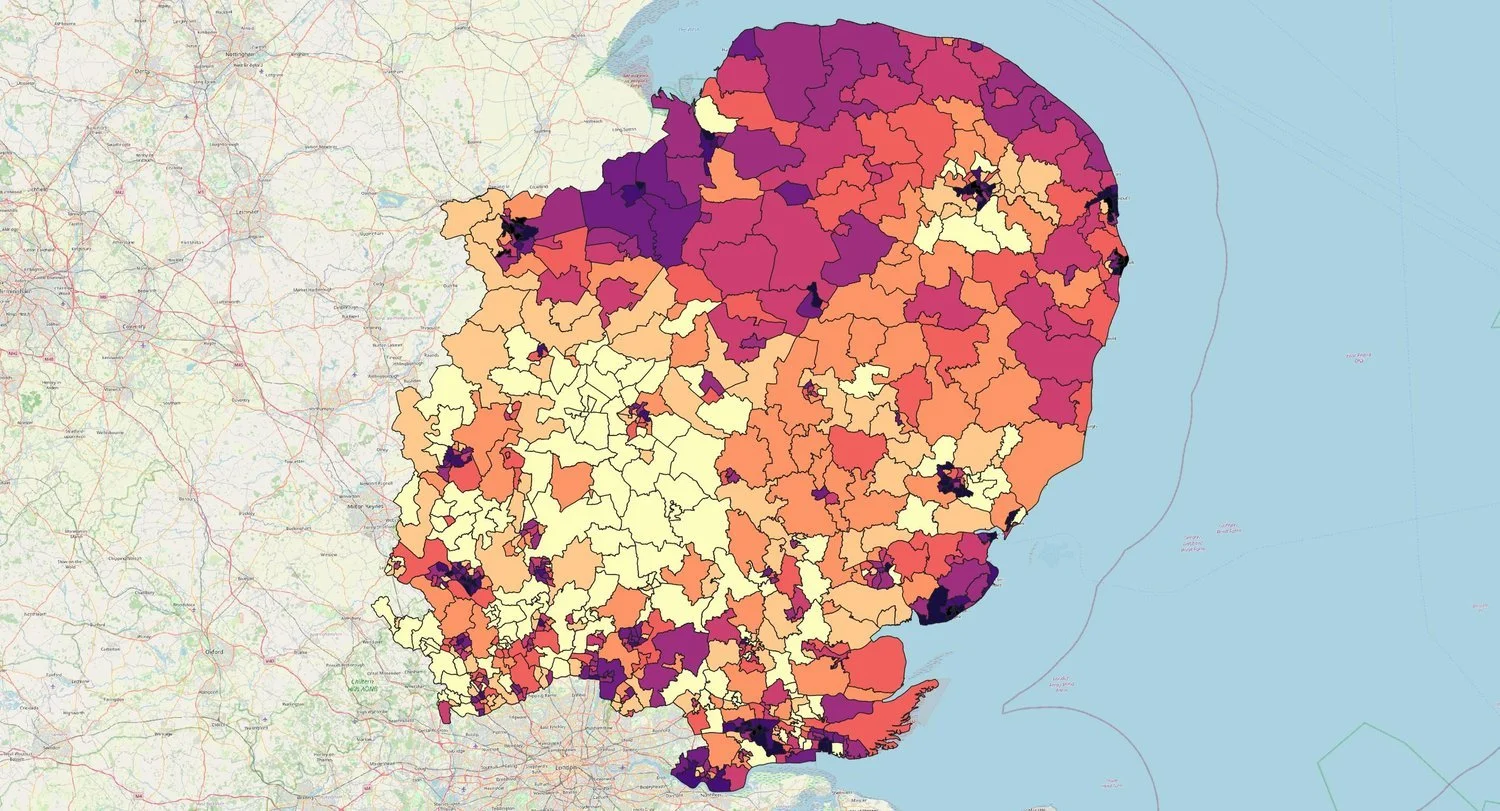
![]()
Top 5 areas of highest biological inequity in East of England:
City Centre West, Norwich
Paston, Peterborough
North Bretton & Westwood, Peterborough
Millfield & Bourges Boulevard, Peterborough
Orton Malborne & Goldhay, Peterborough
-
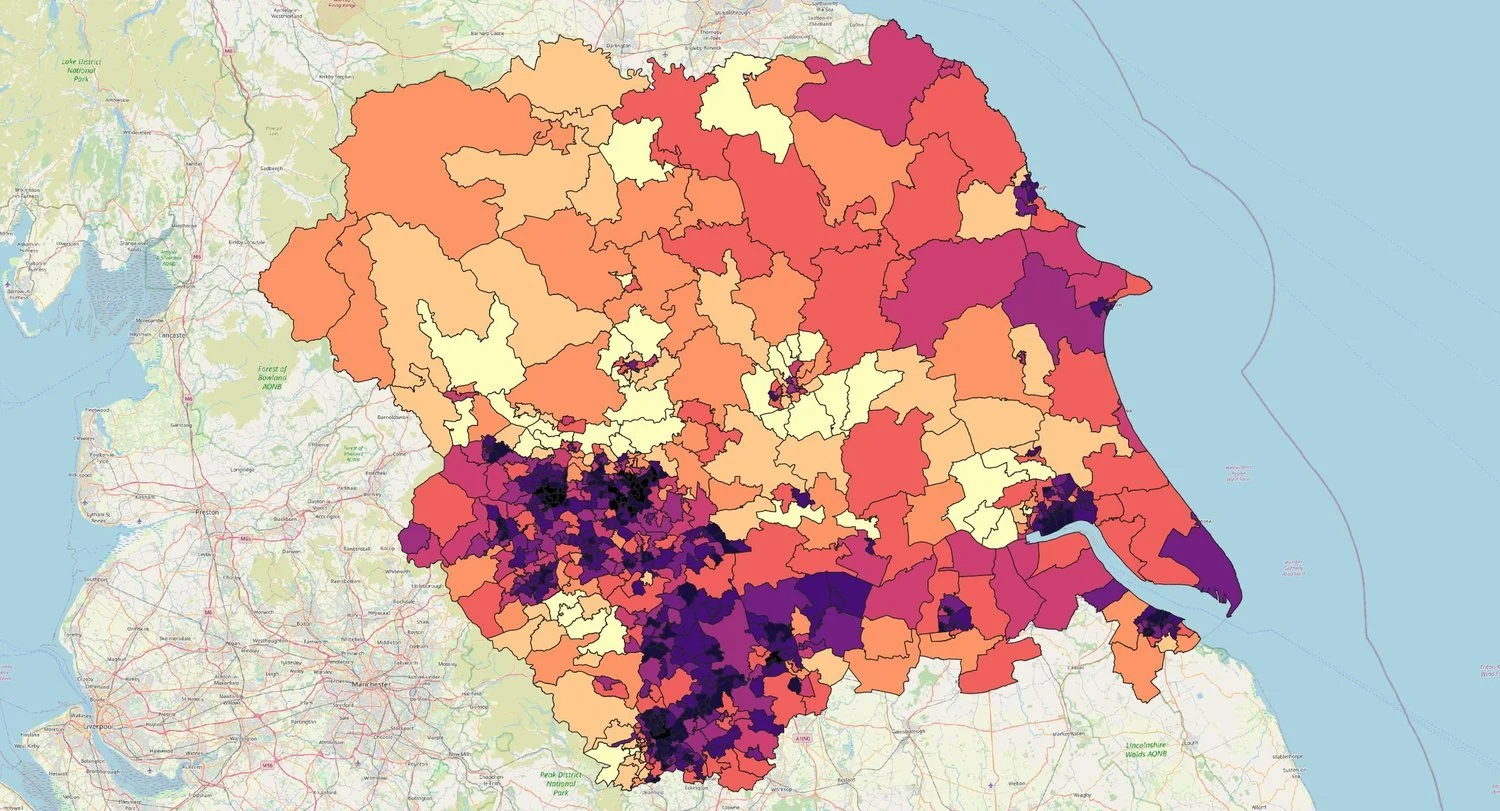
![]()
Top 5 areas of highest biological inequity in Yorkshire & Humberside:
Lincoln Green & St James, Leeds
East End Park & Richmond Hill, Leeds
Central Doncaster & Hyde Park, Doncaster
Burngreave & Grimesthorpe, Sheffield
Central Bradford & Barkerend West, Bradford
-
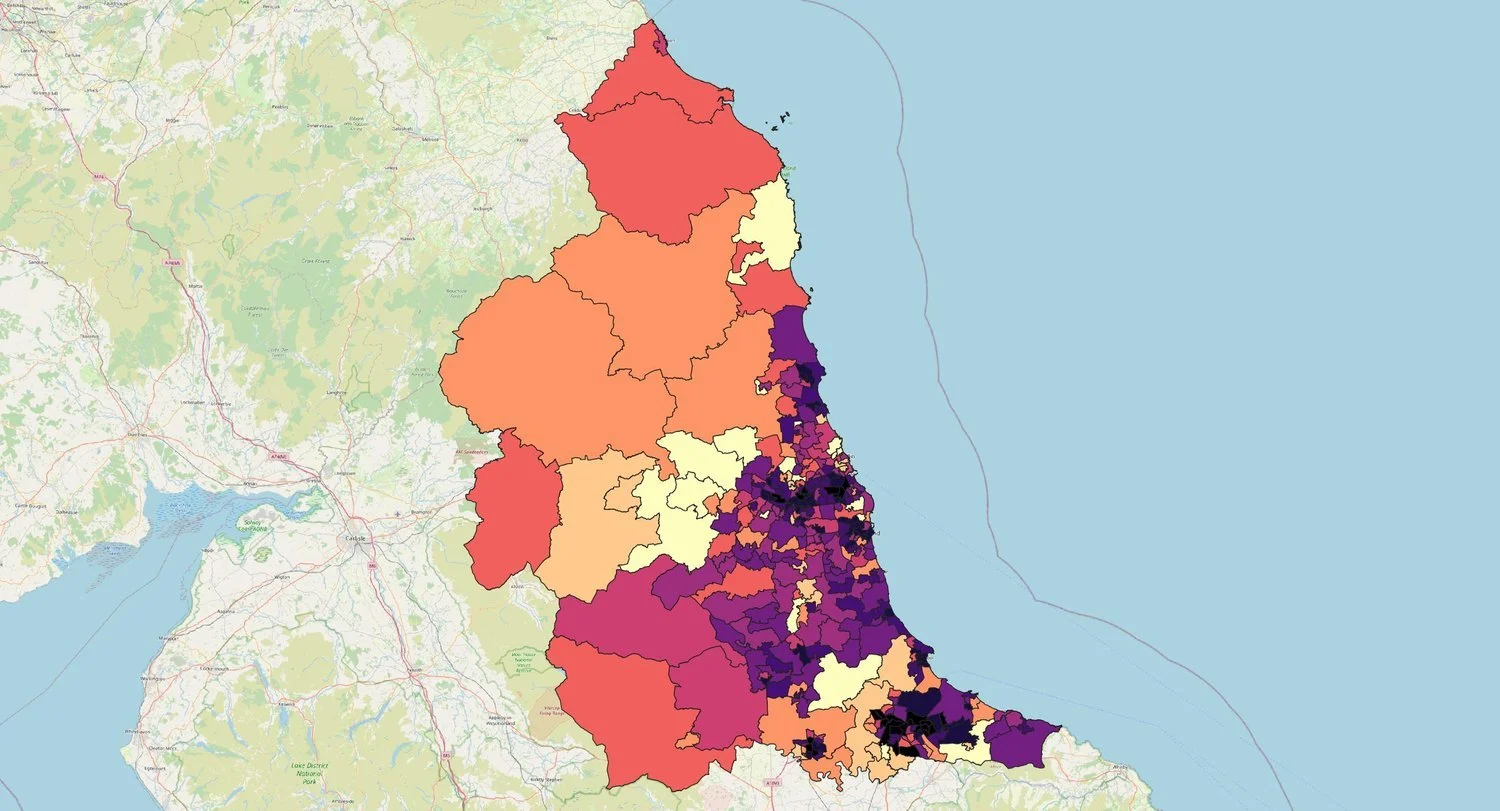
![]()
Top 5 areas of highest biological inequity in the North East:
Middlesbrough Central, Middlesborough
North Ormesby & Brambles, Middlesborough
Ayresome, Middlesborough
Thornaby North, Stockton-on-Tees
Byker, Newcastle-upon-Tyne
-
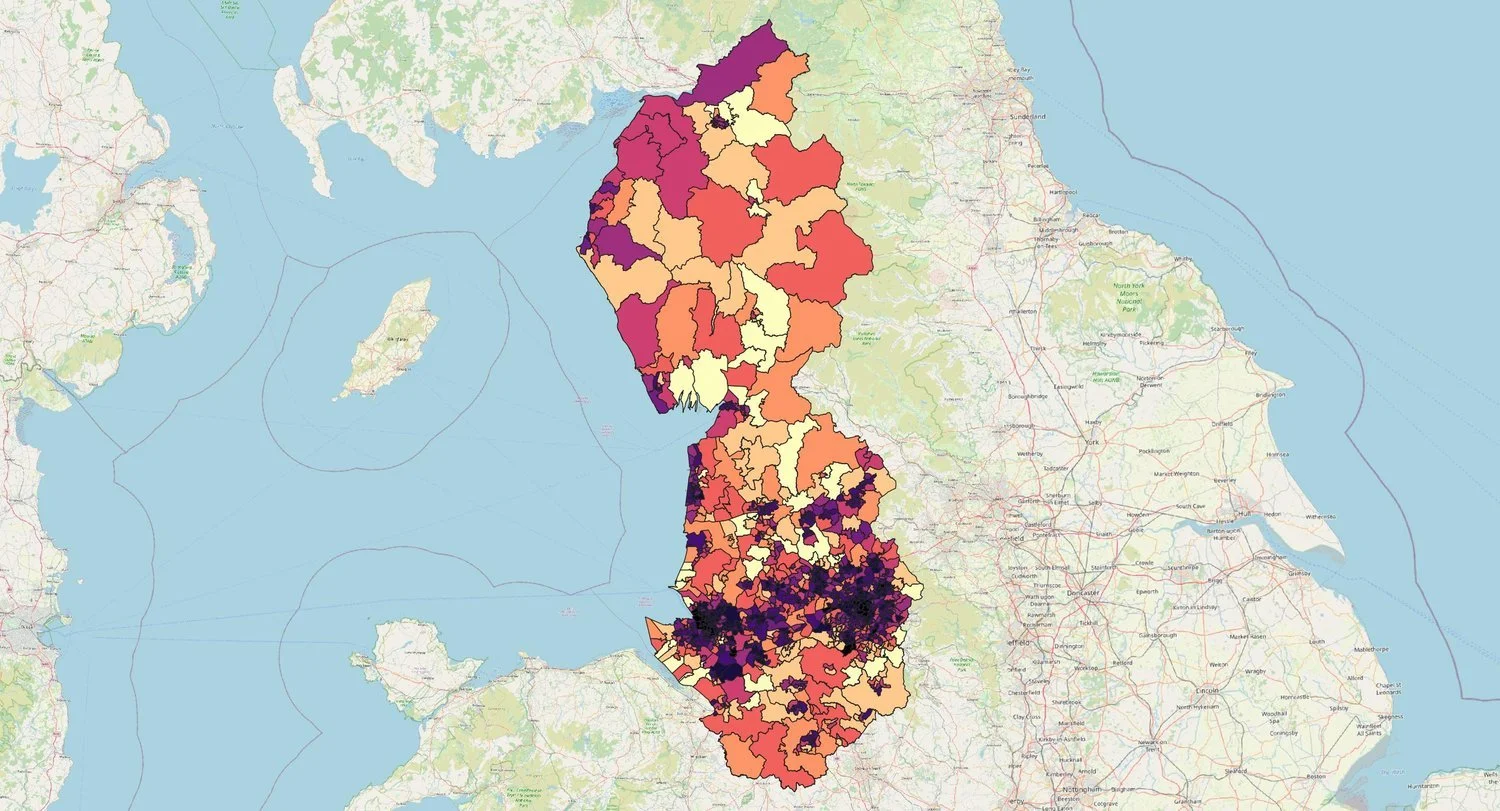
![]()
Top 5 areas of highest biological inequity in the North West:
New Islington & Miles Platting, Manchester
Newton Heath, Manchester
Beswick, Eastlands & Openshaw Park, Manchester
Ardwick, Manchester
Belle Vue & West Gorton, Manchester
-
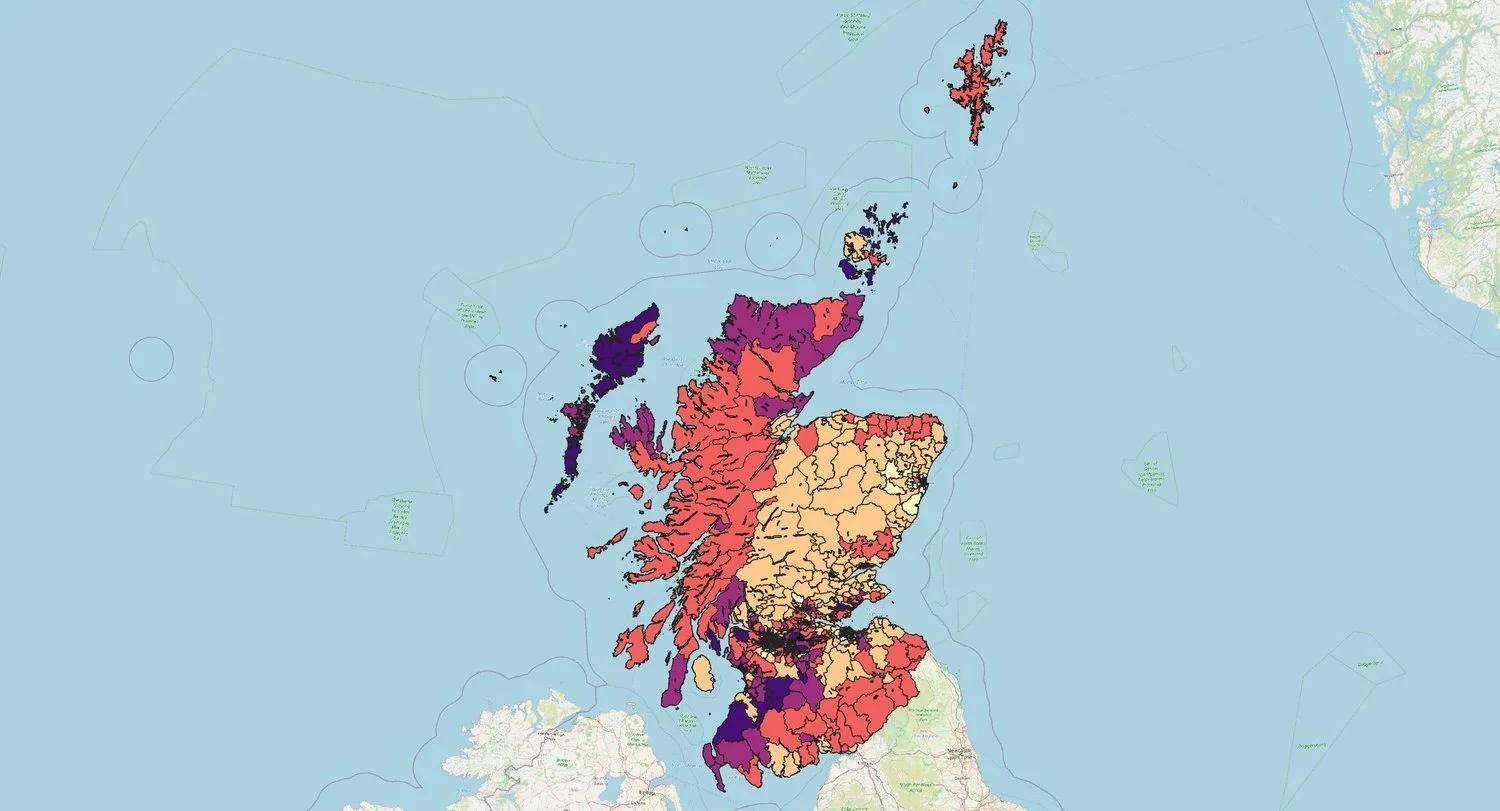
![]()
Top 5 areas of highest biological inequity in Scotland:
Niddrie, Edinburgh
Buckhaven, Denbeath and Muiredge, Fife
Methil West
Methil East
Carnwadric West, Glasgow
-
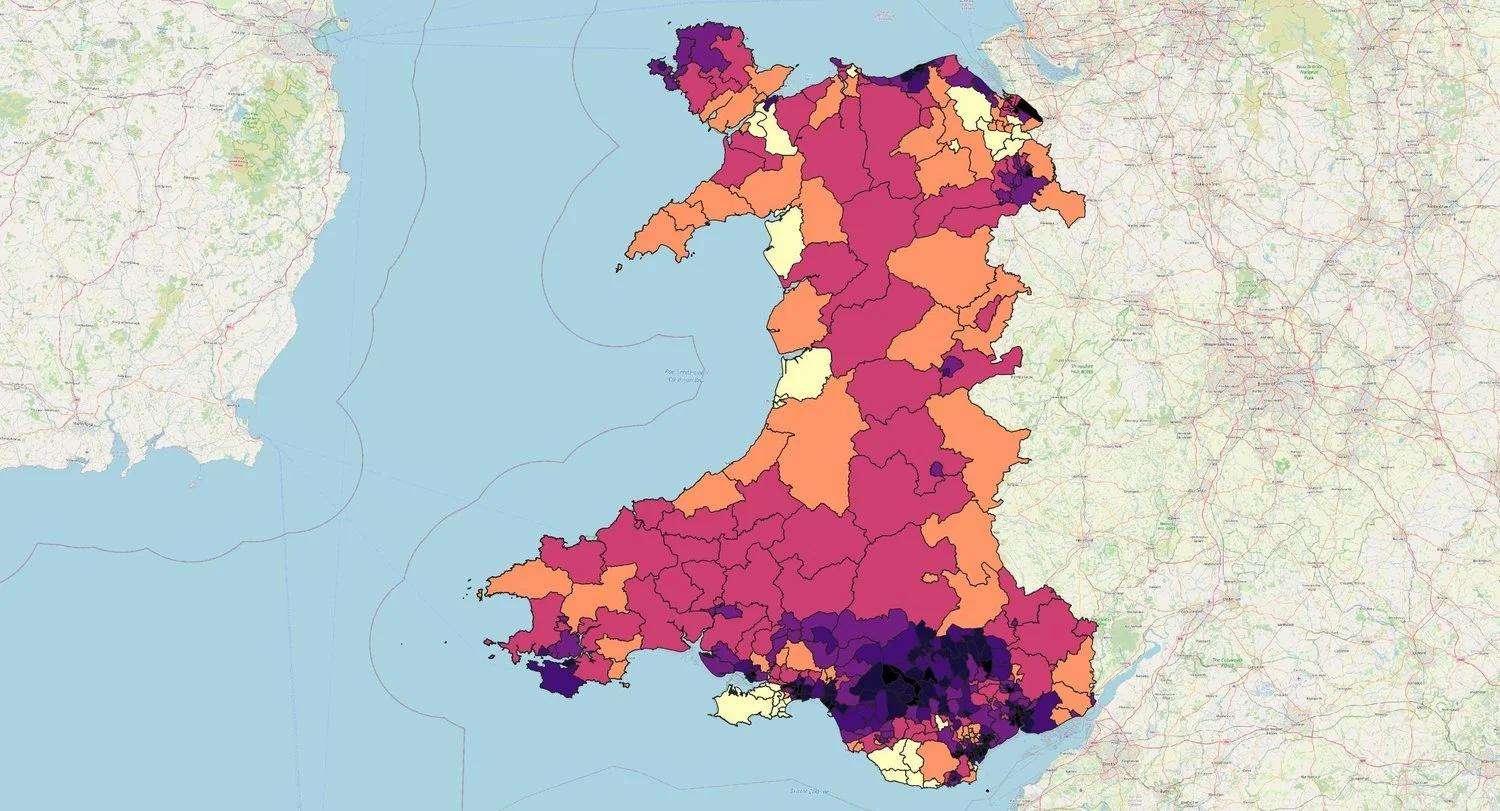
![]()
Top 5 areas of highest biological inequity in Wales:
Swansea 031
Flintshire 018
Ceredigion 001
Ceredigion 002
Swansea 020

ACTION POINTS
For this data to be used in
Spatial Planning and Local Government Planning Policy
To design Local Plans, Supplementary Development Guidance and other policy guidance that regulates the built environment, construction and urbanisation sectors to have achievable targets related to their own actions.
GP Medical Care
For GPs to make note of the environment in which a person lives when communicating health outcomes.
Social Justice work
For campaigns to be emboldened by the truths that where we live influences our biological systems, impacting already marginalised groups the hardest.
